The Rotator Cuff
If you have had shoulder pain, if it very likely that you have heard of the term rotator cuff. You may have even had a scan which showed a problem with the rotator cuff muscle or tendon.
But what exactly is the rotator cuff and is it actually responsible for the pain that you feel in the shoulder?
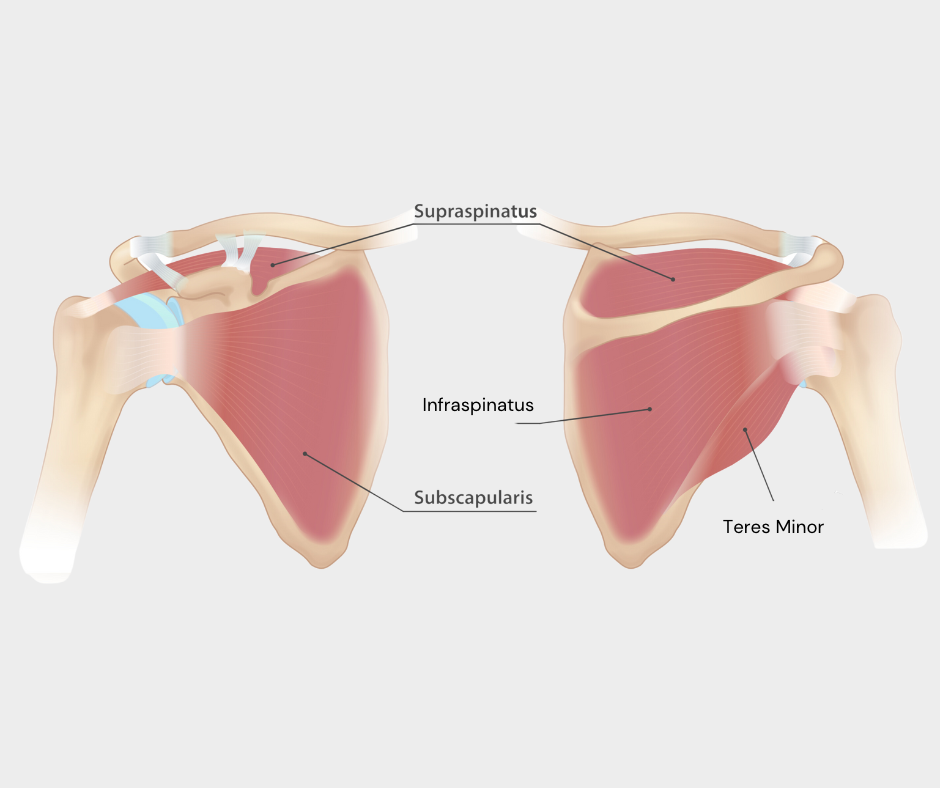
The term rotator cuff refers to a group of 4 muscles which sit on the scapula (shoulder blade) and insert into the humerus (arm bone).
To simplify things the main function of the rotator cuff is to stabilise the shoulder as we raise our arm up, or complete functions such as pushing, pulling, lifting and carrying.
A little bit of history…..

Many of the theories used by physiotherapists and other heath professionals regarding rotator cuff related shoulder pain are actually derived from research by an Orthopaedic Surgeon called Charles Neer, over 50 years ago!
Amongst Dr Neers beliefs was the theory that because the rotator cuff tendons run through a very small gap between the humerus and part of the scapula called the acromion, they could become impinged, especially when lifting the arm overhead. He believed that continual impingement over time leads to degeneration and eventually tears of the rotator cuff tendons.
Historically physiotherapy treatment has focused around strengthening the rotator cuff muscles and increasing the gap between the humerus and acromion. Dr Neer himself invented a surgical procedure called an acromioplasty (one of the most common surgical procedures ever!) which involves shaving away part of the shoulder blade to increase the gap between the ball and socket.
However, more recent research has led to us questioning just how accurate these theories actually are and the theory of shoulder impingement is now subject to controversy and contention .
Studies have shown;
1) No significant differences in outcomes between acromioplasty and sham surgery (pretend surgery) in those diagnosed with shoulder impingement
2) No significant differences in the size of the gap between the ball and socket in those with and without shoulder pain
3) That contact between the humerus and acromion occurs in around 45% of all people but that this does not increase the risk of them developing shoulder pain.
We also know now that findings such as rotator cuff tendinopathy or tears are very common. In fact up to 50% of 60 year olds may have a rotator cuff tear with many of these being asymptomatic.
So if its not my rotator cuff then what is it?
Before we go any further it is important to clarify that this blog post is talking about atraumatic shoulder pain. Injuries that have occurred because of a trauma such as a fall, or a blow to the shoulder are a totally difference subject.

In regards to atraumatic shoulder pain, as stupid as it may sound, being totally honest, in many cases……. WE DON’T ACTUALLY KNOW WHICH EXACT TISSUE IS CAUSING THE PROBLEM!!!!
We used to think that there were a number of special tests we could do to work out which exact tissue was causing the problem. However, we now know that these tests are nowhere near as accurate as we thought they once were.
Whilst there are definitely exceptions that a competent physiotherapist will be able to pick up on, it is more useful to think of MOST atraumatic shoulder problems as fitting into 3 broad categories.
1) Stiff Shoulders
2) Weak Shoulders
3) Unstable Shoulders
Our Role As Physiotherapists Has Changed!
Trying to work out the exact cause of shoulder pain and prescribing exercises targeted at certain structures seems like a logical way to approach things.
However studies suggest that this may not be all that effective. Indeed, in one study of individuals diagnosed with painful rotator cuff tendinopathies, doing rotator cuff strengthening exercises was no better at reducing pain than doing general exercise!
What this shows isn’t that physiotherapy is ineffective, it’s that the answer is more much complex than just strengthening and that we need to do better than just focusing on scans and individual tissues.
The Principal of Settling Down and Building Up
Your physiotherapist should consider all the factors that contributed to the onset of your shoulder pain.
Some examples of these could be:
1) Lifestyle - Starting a new job that involves heavy lifting, increasing volume or intensity of a gym routine or drinking or smoking.
2) Physical - Stiffness in the neck or back or weakness of muscles in the shoulder or back
3) Psychological - A painful shoulder becoming a painful-stiff shoulder due to lack of movement
4) Pain mechanism - For example working out if your shoulder is in an inflammatory state
5) Health - Having certain medical conditions such as diabetes can predispose you to certain shoulder problems

Identifying the contributing factors allows us to come up with strategies to reduce your pain. Once pain is under control we then use these same factors to come up with a plan to build you up again. Either to reduce the chances of pain coming back, or to better manage any ongoing symptoms.
By treating you as an INDIVIDUAL and not as a scan or body part it means that physiotherapy rehabilitation is tailored to your individual needs.